Acoustic neuroma is a non-cancerous growth that develops on the nerve that connects the ear to the brain. This nerve controls both hearing and balance. The tumor grows slowly and usually starts near the inner ear.
The exact cause isn't always known, but in some rare cases, it may be linked to a rare genetic condition(neurofibromatosis type 2 (NF2)). Most people with acoustic neuroma are between 30 and 60 years old.
What is an Acoustic Neuroma?
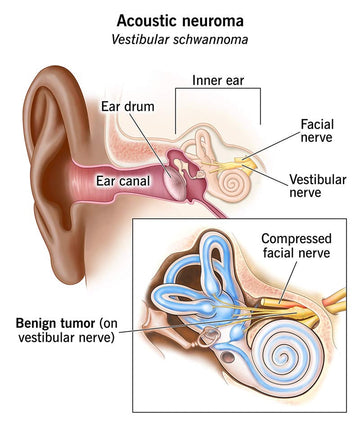
Acoustic neuroma, also known as vestibular schwannoma, is a noncancerous and slow-growing tumor that develops on the vestibular nerve. This nerve transmits balance and hearing signals from the inner ear to the brain.
This tumor forms on the Schwann cells, which are the protective cells that wrap around nerves and help them send signals efficiently. In acoustic neuroma, these cells begin to grow abnormally, forming a tumor. Although the acoustic neuroma grows slowly, it can eventually cause problems by pressing on nearby nerves that affect hearing and balance.
Most cases are not inherited. Around 95% of patients have the sporadic, unilateral type, which means the tumor grows on only one side of the head and is not linked to genetics. The remaining 5% of cases are genetic and bilateral, meaning tumors develop on both sides and are often associated with a rare condition called neurofibromatosis type II (NF2).
In many cases, the tumor stays small and does not grow large enough to press against the brain, but even a small tumor can still affect hearing and balance. Early detection is important for managing symptoms and deciding on the best treatment path.
Symptoms
As mentioned earlier, acoustic neuromas grow slowly, so symptoms often appear gradually and may go unnoticed at first. However, as the tumor begins to affect the surrounding nerves and structures, the following symptoms may occur:
-
Hearing loss (gradual and usually on one side):
This is the most common symptom. It occurs as the tumor presses on the hearing portion of the vestibular nerve. Sudden hearing loss is rare but possible. -
Tinnitus (ringing or buzzing in the ear):
Often experienced in the affected ear, even when there’s no external sound. -
Loss of balance or unsteadiness:
Patients may feel off-balance or tend to fall toward the side where the tumor is growing, especially in the dark or on uneven ground. -
Dizziness or vertigo:
Caused by the tumor interfering with the inner ear’s balance signals. -
Facial numbness or tingling:
This can happen if the tumor presses on the facial nerve, which runs close to the vestibular nerve.
If the tumor becomes large, it can cause increased pressure inside the skull, leading to:
-
Persistent headaches:
Especially when the tumor presses on the dura, the outer membrane covering the brain. -
Blurred or double vision:
Often temporary and caused by fluid buildup in the brain (hydrocephalus), which raises pressure inside the skull. -
Ataxia:
Difficulty with coordination and movement control, leading to clumsy or unsteady movements. -
Voice changes or trouble swallowing (dysphagia):
Occurs when the tumor presses on nerves that control the throat and vocal cords.
Not everyone will experience all of these symptoms, but noticing the early signs, especially hearing loss and balance problems, can lead to earlier diagnosis and better outcomes.
Understanding the Audiogram

An audiogram is a visual chart used to show how well you hear sounds across different pitches (frequencies) and volumes (decibels). It’s a standard tool used in diagnosing hearing conditions like acoustic neuroma.
In the audiogram above:
-
O marks represent the left ear, and
-
X marks represent the right ear.
This specific audiogram reveals:
-
A noticeable difference between the ears, especially in higher frequencies.
-
The left ear (O) shows moderate-to-severe hearing loss, especially from 1000 Hz upward, with a pure tone average (PTA) of 53 dB.
-
The right ear (X) shows milder hearing loss, with a PTA of 33 dB.
-
Speech discrimination (SD) is also affected: the right ear has only 64% word recognition, while the left performs at 100%—a classic sign of nerve involvement rather than just volume-based loss.
-
The Speech Reception Threshold (SRT) is higher in the right ear (50 dB) than the left (30 dB), meaning louder speech is needed to understand words in the more affected ear.
Asymmetrical hearing loss, especially when one ear struggles to understand words clearly even if it hears sounds, is a key red flag for acoustic neuroma. It suggests that the nerve itself is compromised, not just the ear’s sensitivity to sound.
Diagnosis and Treatment
Diagnosing an acoustic neuroma usually starts with a hearing test (audiometry). During this test, you wear headphones and listen to different sounds and spoken words. It helps the doctor check how well you can hear and understand speech in each ear. Hearing loss in one ear, especially when it’s gradual, is often the first sign that something may be wrong.
If the hearing test raises concerns, the next step is usually an MRI scan, which provides detailed images of the brain and inner ear. MRI is the preferred method because it can clearly show if a tumor is present. In some cases, a CT scan may be used instead, especially if an MRI isn’t an option.
Treatment Options
Not everyone with an acoustic neuroma needs immediate treatment. The best approach depends on:
-
The size and position of the tumor
-
How quickly it's growing
-
The person’s age and overall health
-
Whether the tumor is causing symptoms
Treatment options include:
1. Observation
Because acoustic neuromas are usually slow-growing, doctors may recommend regular checkups and MRI scans to monitor the tumor, every 6 - 12 months. This is common when the tumor is small, not causing symptoms, or if the person is older or not in good health.
2. Surgery
Surgery may be recommended if the tumor is large, growing, or causing symptoms like balance problems or facial numbness. The goal is to remove the tumor while protecting nearby nerves, especially the ones that control the face and hearing. While hearing can’t always be saved, surgery often removes the tumor.
3. Radiation Therapy (Stereotactic Radiosurgery)
This is a non-invasive treatment that uses targeted radiation to slow or stop the tumor’s growth. It’s often used for smaller tumors or when surgery isn’t a good option. It doesn’t remove the tumor, but it helps prevent it from getting worse.
It’s important to note that if hearing is already damaged before surgery, it cannot be restored afterward. In such cases, patients may need to use a hearing aid or explore other hearing support options to manage the loss. That’s why early diagnosis plays a key role in treatment outcomes.
Also, remember that many of the symptoms associated with acoustic neuroma; hearing loss, dizziness, or balance issues, can also be caused by other, middle and inner ear conditions such as cholesteatoma or Meniere’s disease. If you’re experiencing more than one of these symptoms, especially if they don’t go away or get worse over time, it’s a good idea to talk to your doctor. They can help determine whether further testing is needed.
Acoustic neuroma is a rare, noncancerous tumor that affects the hearing and balance nerve. While it grows slowly and often causes mild symptoms at first, early detection can make a big difference in how it’s managed. Whether it’s regular monitoring, radiation, or surgery, there are treatment options available to help control the tumor and protect your quality of life.
If you're concerned about symptoms like hearing loss, ringing in the ears, or balance problems, don’t ignore them, getting checked out is the first step toward peace of mind and proper care.